Otitis Media (Middle Ear Infections)
Otitis media is an infection of the air space behind the eardrum, which we call the middle ear. It is one of the most common illnesses of childhood, but may affects persons of any age. It results in over 3 million patient visits annually in the United States alone, and over 4 billion dollars are spent on its treatment every year. Almost 1 million sets of tympanostomy tubes are placed for the treatment of otitis media every year, making this the most commonly performed surgical procedure in the United States. It is likely that someone in your family or someone you know has recently suffered an episode of otitis media.
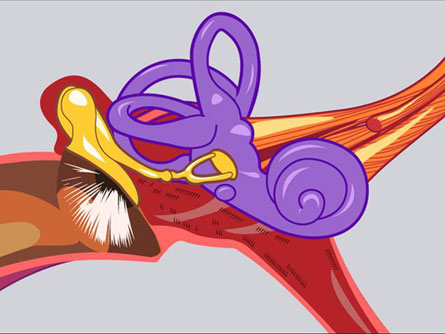
Normal Middle Ear
EAR INFECTIONS AND EUSTACHIAN TUBES
Middle ear infections (otitis media) generally occur because of improper function of the Eustachian tube.
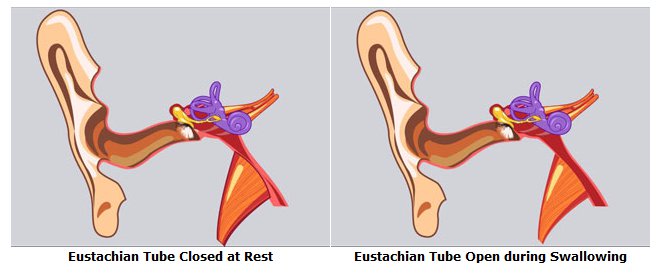
Normal Eustachian tube function: The Eustachian tube connects the middle ear space to the back of the nose. It is usually closed and opens up every time we swallow to equalize the pressure between the middle ear and the air around us. There is air trapped behind the eardrum and that air comes from the atmosphere, which is about 70% nitrogen. The capillaries in the mucosal lining of the middle ear contain blood, which has a concentration of nitrogen of only around 40%. The concentrated nitrogen in the middle ear space diffuses into the nitrogen-poor blood circulating through the middle ear lining, causing a negative pressure or vacuum effect in the middle ear. Fortunately, when we swallow, muscles attached to the Eustachian tube opening in the back of the nose open the Eustachian tube and allow a small bubble of air in to replace the gas which was just absorbed and carried away. This equalizes the pressure for the moment, but the diffusion of nitrogen continues, and the pressure will fall again. Fortunately, we swallow hundreds of times every hour, so middle ear pressures don ?t become extreme or bothersome.
Try swallowing now and listen for the clicking sound in your ears. Go ahead, try it. The clicking you just heard is the sound of the wet walls of the Eustachian tube opening up away from one another and closing again. Some people are astonished to hear the sound, which is actually quite loud, and which occurs hundreds of times an hour when we swallow. Some people do not hear the sound of the Eustachian tubes opening when they swallow and many of these people have problems with their Eustachian tubes and their ears.
Eustachian tube dysfunction: The most common reason for Eustachian tube problems is swelling of the lining of the Eustachian tube, which causes it to remain closed, even though the muscles of the throat are attempting to open it while swallowing. This kind of swelling in the Eustachian tube is commonly caused by common upper respiratory infections and by allergy. Even anatomic differences between individuals may make some more prone to Eustachian tube problems than others.
Another common cause of Eustachian tube problems has to do with the muscles of the throat which open the Eustachian tube. In infants under two years of age, the muscles which open the Eustachian tubes (the tensor veli palatini muscles) do not have an optimal angle of insertion to open the Eustachian tubes during swallowing. As the child’s head grows, however, the angle of the Eustachian tube changes and the tensor veli palatini muscles can open the Eustachian tubes more effectively. This is the reason many infants who suffer from recurrent ear infections grow out of their ear infections around two years of age. In children with a cleft palate, the tensor veli palatini muscles do not anchor to one another in the midline because of the cleft. Because the muscles are not anchored to one another, they cannot pull effectively. Even with surgical repair of the soft palate, these children will often have recurrent middle ear infections which can be prevented by the placement of tympanostomy tubes.
TYPES OF OTITIS MEDIA
Different forms of otitis media have different names depending on the type of fluid that fills the middle ear. Each type differs in its behavior, but none exist without Eustachian tube dysfunction. Some types precede or follow other types as a part of a natural progression.
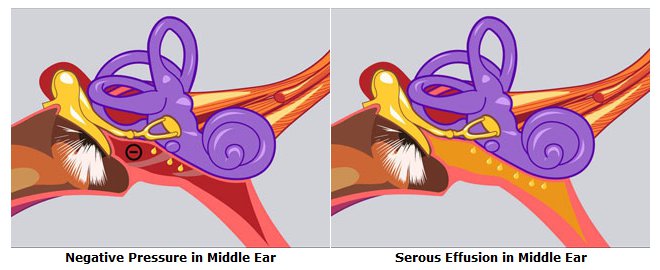
Serous otitis media: So what really happens if the Eustachian tube doesn’t work? If air cannot get in through the Eustachian tube to replace the nitrogen which has been absorbed, then the pressure in the middle ear space will continue to fall. The pressure pulls inward on the eardrum and on the first hearing bone (the malleus), causing the chain of hearing bones to become stiff and the hearing muffled. This is the way you feel when you are descending down a large hill or a mountain in your car or descending in an airplane and you cannot get your ears to pop. The negative pressure on the eardrum can become so strong that the sensitive eardrum is stretched, creating pain. At times, the eardrum will rupture, allowing air in and equalizing the pressure. If the negative pressure gets great enough and stays for long enough, it will actually suck blood out of the capillaries in the lining of the middle ear. The blood cells, however, get held back by the walls of the capillaries which are built like a fishnet, but the yellow protein and sugar-filled fluid between the cells, the serum, can pass through the capillary walls and fill the ear. We call this condition serous otitis media, because of the serous fluid in the middle ear.
The eardrum does not work very well when the middle ear behind it is filled with fluid because sound will bounce off the surface of the fluid, just as it bounces off the surface of the water in the swimming pool, preventing us from hearing sounds above. Because the middle ear also has a mechanical sound conduction mechanism (the hearing bones, or ossicles), the amount of hearing loss caused by serous otitis media can vary greatly from individual to individual.
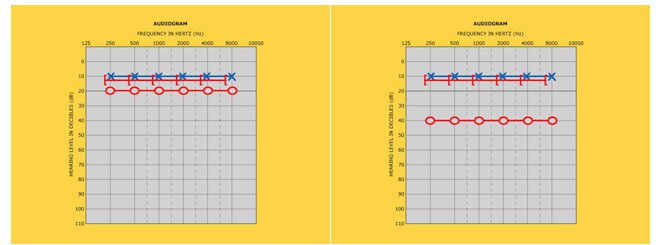
These graphs of hearing (audiograms) both show a normal hearing line across the top of the graph for the left ear shown in blue. If the right ear (shown in red) is filled with fluid, a blockage of sound entry results in varying amounts of hearing loss. The hearing loss on the audiogram on the left is mild. On the right, the hearing loss is moderate.
The fluid in the ear does not necessarily cause pain, and it may sit around for weeks or months before resolving. Usually, this happens when the underlying cause of the swelling in the otherwise normal Eustachian tube has diminished. In an adult, serous otitis media is very disturbing because of the hearing loss it causes, so physicians will generally prescribe some combination of decongestants, antihistamines, or steroids to reduce swelling in the Eustachian tube and promote drainage of the fluid. Many adults feel so impaired by their temporary hearing loss that they will choose to have the fluid drained by an otolaryngologist in the office. In a child, the fluid may be present without causing pain, and can cause hearing loss which the few children will complain about. Over periods of months and years, this can lead to delays in speech, language, and learning. Children will not learn to pronounce sounds that they cannot hear, and they cannot attend to spoken instruction they cannot hear. In children with persistent fluid in the middle ear causing hearing loss, speech problems, or language delays, the option of placement of tubes to eliminate the possibility of serous otitis media is generally discussed.
Acute otitis media: If middle ear fluid persists, bacteria may enter this nutrient-rich space and continue to reproduce and the lining of the middle ear will begin to swell. The body then recruits millions of white blood cells to fight the infection. This results in an abscess with outward pressure on the sensitive eardrum and the swollen middle ear lining, causing a pulsing pain. We call this condition acute otitis media. Antibiotics can kill bacteria and stop symptoms but usually take one day or more to reduce symptoms. The most efficient treatment of an abscess is drainage and, sometimes, the eardrum will rupture, allowing the infection to drain. More commonly, the infection will drain naturally down the Eustachian tube. The swollen walls of the middle ear lining collapse the space and force the infected material out. This begins the resolution of the infection.
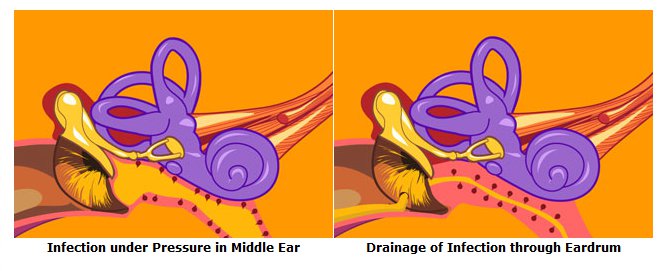
Contrary to popular belief, the eardrum does not rupture like a balloon, resulting in total loss of the eardrum. The eardrum is more like the paper cone of a speaker, and when the pressure gets too great behind it, it may burst in one small spot, relieving this pressure. This tiny pinhole perforation will usually close within a few hours. Antibiotics are normally given by this point (or before) to help clear up the infection. In an adult, if the infection does not start to resolve within a day or two on antibiotics, the eardrum may be lanced in the office to allow the infection to run out. This usually results in a rapid resolution of the infection. That might be the end of the infection, but if the Eustachian tube continues to not work well (from allergy, abnormal anatomy, or other factors), the cycle of negative pressure, buildup of fluid and infection will repeat itself again.
Secretory otitis media: At times, after an episode of acute otitis media is treated with an antibiotic, the acute, painful portion of the infection will resolve, but the middle ear will remain filled with a thick, mucous-like fluid that the cilia of the middle ear lining has great difficulty getting rid of. The fluid may persist for months, filling the middle ear and causing a significant hearing loss. It may even be difficult to see the fluid when looking in from the outside. This condition is called secretory otitis media. Secretory otitis media is a real worry because it also tends to be silent, that is, not associated with any pain or fever, but can result in a significant hearing loss, which, if undetected, can profoundly affect normal speech and language development in a young child. If secretory otitis media with hearing loss is present and fails to respond to antibiotics, tympanostomy tube placement is usually recommended to reverse hearing loss.
TYMPANOSTOMY TUBES

Tube in Eardrum
In patients with repeated episodes of acute otitis media or persistent middle ear fluid, doctors will often recommend placement of tubes in the eardrums, whose purpose is to allow air to enter the middle ear to replace that which is absorbed by the lining of the middle ear itself. The pressure always remains equalized this way. When pressure remains equalized, the negative suction pressure which results in fluid buildup in the middle ear is prevented, and so are the infections. It is another common misconception that the tubes placed in the eardrum are placed as drains, when in fact, they are there for pressure equalization.
The tympanostomy tubes placed in eardrums today may have long or short shafts, wide or narrow bores, and may be made of a range of different plastics, stainless steel, or even titanium. Some tubes even have antibiotics impregnated onto their surface, in an effort o reduce infections that sometimes occur after tube placement. The type of tube used, however, is generally the surgeon’s preference and is much less important than the decision to place or not to place tubes in the first place.
In any person over 10 years of age, a tube can usually be placed in the eardrum in the office, but in younger children, the tubes are more easily placed in the operating room under anesthesia. The tubes themselves tend to come out 6 months to a year later. This is because they get swept up in the current of migrating epithelium on the drumhead, are pushed to the edge of the eardrum, and finally pulled out. This outward migration of epithelium is the reason tubes generally do not fall into the middle ear. If, after extrusion of the tubes, infections recur, the tubes can be replaced. If children do not grow out of their Eustachian tube problems by 2 years of age, they tend to outgrow them by 6 or 8 years of age. Some patients with Eustachian tubes that do not work well will continue to have Eustachian tube problems their entire lives, and will always feel better, hear better, and have fewer infections with tympanostomy tubes in their eardrums at all times. In these patients, recurrent tympanostomy tube placement may be inconvenient and specialized tubes called T-tubes can be placed, which may last 18 months to 2 years, or sometimes even longer. The convenience of having long-lasting tubes in place has to be weighed against the small risk that a hole in the eardrum will develop at the site of the tube.
Water and tympanostomy tubes: There has always been a great deal of concern about water and the presence of ear tubes, and it has been a common, traditional practice to prohibit all water entry into the ear in persons who have tympanostomy tubes in place. The reason for this is that even with tubes in place, it is possible for children to get occasional ear infections, likely from infection that ascends from the back of the nose into the middle ear along the Eustachian tube. These infections often seem even worse than the painful infections that occurred prior to tube placement, because with a tube in the eardrum, the infection runs out, making a smelly and worrisome mess. These infections usually clear up quickly with antibiotics and with antibiotic drops which can enter the tube and quickly decontaminate the middle ear.
It was easy for doctors to attribute these infections to water which had gotten into the middle ear through the tympanostomy tube, so children were forced to wear earplugs while swimming. Children who continued to get ear infections, even with earplugs, were forced to wear bathing caps on top of their plugs or even kept out of the water altogether. In recent years, it is becoming more and more recognized that water, especially chlorinated pool water, poses little risk of infection to children with tympanostomy tubes. Children are commonly allowed to swim freely without plugs, but in some areas, may be asked not to dive deeper than 5 or 6 feet. There continues to be more caution with less-clean water, such as ocean, lake, pond, or river water, which carries a higher concentration of bacteria and other unusual microorganisms. In some areas, children swim without plugs but are told to use antibiotic ear drops in the evening before going to bed. As you can see, there is a wide variety of policy regarding this issue. Your physician will tell you what he or she feels most comfortable with.
COMPLICATIONS OF OTITIS MEDIA
There are many negative consequences of recurrent or severe middle ear infections or persistent Eustachian tube dysfunction, including damage to the middle ear (eardrum and hearing bones), damage to the inner ear, and even damage to the brain.
Middle ear injury: With recurrent ear infections, the eardrum (tympanic membrane) may become “scarred.” Scar tissue generally has less blood supply than normal tissue. As such, it is less resistant to infection and eventually, a point may come that the eardrum, when faced with the stress of an abscess, dissolves away, leaving a hole in the eardrum. This leads to hearing loss because the eardrum no longer has the surface area to collect all of the sound coming into the ear.
Repeated infections may also impair the delicate motions of the middle ear bones so that they become stiff or even stuck. This can cause a significant amount of hearing loss because sound collected by the eardrum cannot get passed through the chain of hearing bones to the inner ear. Infections and constant negative pressure can also cause portions of the hearing bones to dissolve so that the continuous chain from the eardrum to the inner ear is broken. Sometimes, the skin that normally migrates out of the ear canal will instead migrate into the middle ear. The skin can migrate through a perforation or be drawn into the ear by negative pressure. This is called a cholesteatoma. This may result in chronic infections with drainage and occasionally pain, and often a very large hearing loss. All of the above problems can be repaired surgically.
Inner ear injury: Recurrent ear infections can also have profound effects on hearing in the inner ear. Toxins from infections can diffuse through a membrane called the round window into the fluids of the inner ear. These toxins can injure the delicate hearing structures in the inner ear, especially in the highest frequencies which are closest to the round window membrane. In severe cases, the hearing and balance function of the inner ear can be lost completely (labyrinthitis), causing permanent deafness in the affected ear and loss of balance function.
Severe complications: The brain lies directly on top of the middle ear and is separated from it by a very thin layer of bone. Infections can spread from the middle ear to the brain through direct erosion of this bone, through pre-existing defects in the bone, through the inner ear, or through nearby blood or lymphatic vessels. The most common intracranial complication is meningitis. This will result in headache, lethargy, neck stiffness, and high fever, as well as occasional seizures. Meningitis from otitis media is generally treated aggressively with surgery and antibiotics. Surgery is performed to drain accessible areas of the infection. Other complications such as a brain abscess can also occur but are fortunately rare.
Information Provided by Dr. Michael Teixido, MD
Dr. Teixido is a board certified Otolaryngologist and Otologist/Neurotologist, with a special interest in medical and surgical conditions that affect hearing and balance. He is actively pursuing his goals of advancing the study and understanding of problems involving hearing and balance as a result of hereditary hearing conditions in his own family. View Dr. Teixido's Full Bio
FOULKSTONE
PLAZA
1401 Foulk Road.,
Suite 205
Wilmington, DE 19803
Phone: (302) 998-0300
Fax: (302) 478-8069
Greenville
Location
1011 Centre Rd,
Suite 200,
Wilmington DE 19805
Phone: (302) 998-0300
Fax: (302) 543-8456
MIDDLETOWN
CROSSING
306 EastMain Street
Middletown, DE 19709
Phone: (302) 998-0300
Fax: (302) 376-5251
NEWARK- IRON HILL
CORPORATE CENTER
700 Prides Crossing
Suite 200
Newark, DE 19713
Phone: (302) 998-0300
Fax: (302) 998-5111